Retake
C17) Pleuritic chest pain and SOB in a young, tall male
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with hypoxia.
- Review the DDx considerations in a patient with hypoxia.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient with hypoxia.
History
A 21-year-old male presents to the ED after one hour of sudden onset, sharp chest pain and shortness of breath. The chest pain is worst when taking deep breaths. He denies any trauma or any past medical history.
Physical Exam
BP: 119/78, HR 102, RR 23, Temp 36.5C, O2 saturation 89%. General: Tall and thin. Pulmonary: Hyperresonance to percussion and diminished breath sounds in the left upper chest. Trachea is midline. CV: No JVD.
Labs
D-dimer: 0.01mg/L (normal <0.50mg/L)
Provisional Diagnosis
Select the Dx you believe is most appropriate
Both pulmonary embolism and spontaneous pneumothorax can present with pleuritic chest pain, dyspnea, and acute onset shortness of breath. Spontaneous pneumothorax is more likely in this young, tall, thin patient without any risk factors for PE with a negative D-dimer.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
This patient merits urgent workup considering the potentially life-threatening etiologies.
First Imaging Study
What is the first imaging study you will order?
Chest X-ray can be obtained quickly, can detect a pneumothorax, and can sometimes suggest pulmonary embolism (Hampton’s hump; rounded opacification secondary to lung infarction).
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
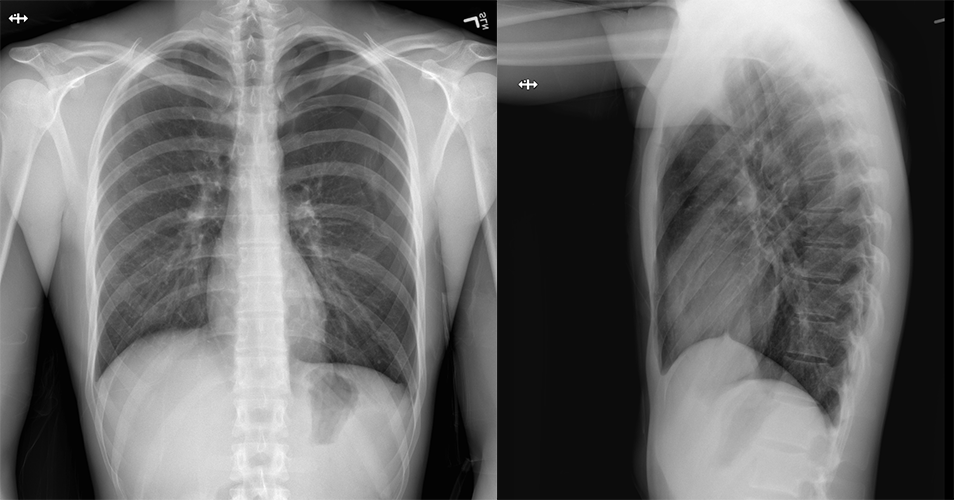
Chest x-ray
What best describes the findings on the Chest X-ray?
There is a visible white pleural line with absent lung markings in the left hemithorax, consistent with a left pneumothorax.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
Further imaging is not required at this time. CT is only necessary if there is a persistent air leak following chest tube placement to assess for a bronchopleural fistula or blebs.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
While imaging suggests a developing tension component, tension is a diagnosis made by the patient's clinical presentation. In this case, there is no tracheal deviation, JVD, or obstructive shock to suggest that there is atension component.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient will require urgent chest tube placement.
Assessment and Plan
Please provide your assessment and plan for this patient
A 21-year-old tall male without any PMH presents with a spontaneous left sided pneumothorax without tension. He will require urgent chest tube placement and admission for chest tube management (chest tube to suction, then water-seal trials following pneumothorax resolution, then removal). The patient will require a chest CT if he develops a persistent air leak.
Lessons Learned:
- A spontaneous pneumothorax may occur in young, tall patients without any significant past medical history.
- A pneumothorax appears on a chest X-ray as absent lung markings beyond the visible visceral pleural line of the affected lung.
- If there is strong clinical suspicion of tension pneumothorax in the setting of trauma, a chest tube should be placed prior to imaging to avoid potentially fatal delays in intervention.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Contributors:
Kevin Pierre, MD - Editor
Robbie Slater, MD - Supervising Editor
Bayar Batmunh, MS - Coordinator
Next


{kind=link}